Am J Transl Res 2025;17(7):5766-5778
943-8141/AJTR0165484
Original Article
Identification of risk factors
and development of a high-performance
predictive model for non-healing in elderly patients
with intertrochanteric fractures post-internal fixation
Jianyue Wu
1*
, Peng Xu
1*
, Dong Zhang
1
, Yingjie Ni
1
, Jijun Zhao
2
1
Department of Orthopedics, Wuxi Xishan People’s Hospital, Wuxi 214015, Jiangsu, China;
2
Department of Ortho-
pedics, Wuxi People’s Hospital, Wuxi 214023, Jiangsu, China.
*
Equal contributors and co-first authors.
Received April 21, 2025; Accepted July 10, 2025; Epub July 25, 2025; Published July 30, 2025
Abstract:
Objective: To identify risk factors associated with non-healing in elderly patients with intertrochanteric
femoral fractures treated with internal fixation and to develop a predictive model for non-union risk. Methods: We
conducted a retrospective analysis of 889 elderly patients treated with internal fixation for intertrochanteric frac
-
tures at Wuxi Xishan People’s Hospital from March 2021 to December 2024. Patients were classified into healing
(n=806) and poor healing groups (n=83) based on radiographic evidence three months post-surgery. Univariate
and multivariate logistic regression analyses were used to identify significant risk factors. A predictive model was
developed and validated using receiver operating characteristic (ROC) analysis and the area under the curve (AUC).
Results: Significant risk factors for poor healing included smoking history (Odds ratio [OR] 1.750, P=0.022), os
-
teoporosis (OR 2.055, P=0.003), posterior or medial wall bone defects (OR 1.964, P=0.005), low postoperative
albumin (OR 1.674, P=0.032), and early weight-bearing (OR 1.765, P=0.018). The use of proximal femoral nail
antirotation (PFNA) significantly reduced the risk of poor-healing (OR 0.515, P=0.006). The combined predictive
model achieved an AUC of 0.949, indicating high predictive value. Conclusions: Our findings highlight key risk fac
-
tors for non-healing in elderly patients post-internal fixation for intertrochanteric fractures. The developed predictive
model, incorporating clinical, biochemical, and surgical factors, offers high accuracy and may help identify high-risk
patients for targeted intervention.
Keywords:
Intertrochanteric fractures, internal fixation, non-healing risk factors, elderly patients, predictive model,
orthopedic surgery
Introduction
Intertrochanteric fractures, occurring between
the femur’s greater and lesser trochanters,
pose a significant threat to elderly patients,
with high rates of morbidity and mortality [1].
These fractures account for approximately half
of all hip fractures in this age group [2]. As life
expectancy increases and the elderly popula
-
tion grows worldwide, the incidence of these
fractures is expected to rise [3]. This trend
underscores the need for better management
strategies for post-surgical care [4].
Internal fixation using devices such as dynamic
hip screws (DHS) or intramedullary nails is the
standard treatment [5]. The goal of surgery is to
restore mobility and function. However, some
patients experience non-healing or delayed
healing after the procedure [6, 7]. Non-healing
refers to the failure of the fracture to unite
within an expected timeframe, resulting in pro
-
longed immobility, persistent pain, and an
increased risk of complications such as non-
union or implant failure [8]. Identifying the
causes of non-healing is crucial for improving
patient outcomes [9].
Previous studies have identified several factors
that may contribute to non-healing in elderly
patients following internal fixation for intertro
-
chanteric fractures [10, 11]. These patient-spe
-

Risk factors and predictive model for non-healing
5767
Am J Transl Res 2025;17(7):5766-5778
cific factors significantly influence the body’s
response to injury and healing [12].
Fracture-related factors, such as fracture type,
displacement of bone fragments, and the de-
gree of comminution, are important for deter-
mining the stability of fixation and the biolo-
gical conditions required for healing [13, 14].
Treatment-related factors, including the choice
of fixation device, timing of surgery, and the sur
-
geon’s skill, also play a crucial role in healing
outcomes [15].
While these risk factors are known, there is a
lack of well-established models to predict
which patients are most likely to experience
non-healing after surgery [15]. Developing such
models requires a comprehensive analysis of
how these risk factors interact and influence
patient outcomes [16]. Advances in statistics
and machine learning offer promising oppor-
tunities to create robust predictive tools that
could greatly enhance clinical decision-making
and individualized patient care [16].
Recent studies using predictive analytics in
orthopedics have shown promising results,
emphasizing the value of integrating various
types of data into unified models [17]. These
models may assist in identifying high-risk
patients prior to surgery, enabling tailored
approaches such as closer postoperative mo-
nitoring, enhanced nutritional support, or per-
sonalized rehabilitation plans. Testing these
models on independent datasets is crucial to
ensure their reliability across different clinical
settings.
This study has two primary objectives: (1) to
identify risk factors for non-healing in elderly
patients following internal fixation for intertro
-
chanteric fractures, and (2) to develop and vali-
date a predictive model based on these fac-
tors. By systematically examining the variabl-
es associated with non-healing, this research
aims to contribute to existing knowledge and
provide clinicians with a practical tool to miti-
gate the risks of non-healing.
Materials and methods
Research design and participants
A retrospective analysis was conducted on
elderly patients who underwent internal fixation
for intertrochanteric femoral fractures at Wuxi
Xishan People’s Hospital between March 2021
and December 2024. Patients were classi-
fied into two groups based on their healing sta
-
tus three months after surgery: a poor healing
group (n=83) and a healing group (n=806).
Fractures were classified as poorly healed if
X-ray images showed visible fracture lines,
breakage of fixation devices, misalignment of
fractures, or loosening or detachment of the
plate from the bone shaft, all indicative of inad-
equate bone healing.
Approval for this study was granted by the
Institutional Review Board of Wuxi Xishan
People’s Hospital. Basic patient information
was obtained from the hospital’s electronic
case records. Since the study involved de-iden-
tified patient data, informed consent was
waived, with this exemption approved by the
hospital’s Ethics Review Committee. Data col
-
lection and analysis followed ethical guide-
lines set by the hospital’s ethics committee.
Selection criteria
Inclusion criteria were as follows: (1) Initial diag-
nosis of intertrochanteric femoral fractures
confirmed through imaging; (2) Underwent
internal fixation surgery for these fractures at
our hospital; (3) Aged 65 years or older; (4)
Availability of complete clinical data.
Exclusion criteria included: (1) Severe organ
dysfunction (heart, lung, liver, or kidney); (2)
Lower limb paralysis or sensory and motor
impairments; (3) Loss to follow-up after sur-
gery or incomplete follow-up; (4) Mental illness
or inability to communicate normally or com-
plete assessments.
Data collection
Baseline data were collected from the hospi-
tal’s case management system, including gen
-
der, age, body mass index (BMI), fracture type,
and underlying conditions such as diabetes
mellitus, hypertension, and osteoporosis. Addi-
tional socioeconomic data, including ethni-
city, educational level, and monthly household
income, were also gathered.
Blood samples (5 ml) were collected before and
after surgery. Hemoglobin and albumin levels
were measured using an automated blood ana-

Risk factors and predictive model for non-healing
5768
Am J Transl Res 2025;17(7):5766-5778
lyzer (Sysmex XN-1000, Japan). C-reactive pro
-
tein (CRP) and interleukin-6 (IL-6) levels were
assessed using an IMMAGE Immunoassay
System (Beckman Coulter, USA). Vitamin D lev-
els were measured with a Waters ACQUITY
UPLC System linked to a Xevo TQ-S tandem
mass spectrometer (Waters Corporation, USA).
Grading criteria
Fracture alignment was assessed using the
Garden alignment index, based on angles
observed in both anteroposterior and lateral
X-rays [18]. Fracture stability was classified
using the Arbeitsgemeinschaft für Osteosyn-
thesefragen (AO)/Orthopaedic Trauma Asso-
ciation (OTA) system [19]. Stable fractures were
classified as A1.1 to A2.1, while highly unstable
fractures were categorized as A2.2 to A3.3.
Preoperative health status was evaluated us-
ing the American Society of Anesthesiologists
(ASA) physical status classification [20]. ASA I
patients were healthy individuals with no coex
-
isting conditions, while ASA II patients had mild
systemic disease without functional limitations.
ASA III patients had moderately severe system-
ic disease with restricted activity, and ASA IV
patients had severe disease with poor car-
diopulmonary function, indicating a moribund
state. No ASA V patients were included in this
study.
Psychological and cognitive assessments
Several standardized tools were used to as-
sess mental health and cognitive function. The
Conners’ Parent Symptom Questionnaire (PSQ)
measured anxiety and behavioral problems,
with higher scores indicating more severe
issues. The Stroop Color-Word Interference
Test assessed attentional inhibitory control,
with lower scores reflecting better performan-
ce. The Wisconsin Card Sorting Test (WCST)
evaluated executive function and adaptability
to changing rules. The Alternate Uses Task
measured cognitive flexibility and creativity by
asking participants to suggest alternative uses
for common objects. The Pittsburgh Sleep
Quality Index (PSQI) assessed sleep quality,
with higher scores indicating poorer sleep. The-
se assessments were conducted preoperative-
ly to explore associations with surgical healing
outcome.
Statistical analysis
Statistical analysis was performed using SPSS
software (version 24.0). Categorical variables
were reported as percentages and frequen-
cies, and comparisons were made using the χ
2
test. Continuous variables were assessed for
normality using the Shapiro-Wilk test; those
conforming to a normal distribution were ex-
pressed as means ± standard deviations (X ±
sd), and group comparisons were performed
using independent samples t-tests. Logistic
regression was used to identify factors influ
-
encing nonunion following internal fixation for
intertrochanteric femoral fractures. Receiver
operating characteristic (ROC) curves were
constructed, and the area under the curve
(AUC) was calculated to evaluate the predictive
accuracy of the risk model. An AUC greater than
0.9 indicates high accuracy, between 0.71 and
0.90 suggests moderate accuracy, and be-
tween 0.5 and 0.7 signifies poor accuracy.
Additionally, Decision Curve Analysis (DCA), cal-
ibration curves, and a nomogram were devel-
oped to assess the clinical utility and predic-
tive performance of the model. Statistical sig-
nificance was defined as a
P
-value <0.05. The
goodness-of-fit for the risk model was evaluat
-
ed using the Hosmer-Lemeshow test, where a
P
-value >0.05 indicates adequate model fit.
Results
Comparison of demographic and basic data
A total of 889 elderly patients with intertro-
chanteric fractures who underwent internal fix
-
ation surgery were analyzed to identify risk fac-
tors associated with poor healing (
Table 1
). No
significant differences were observed between
the two groups in terms of gender distribution,
age, BMI, ethnicity, hypertension, hyperlipid-
emia, educational level, or monthly household
income per person (all P>0.05). However, cer
-
tain factors were significantly associated with
poor healing outcomes. Specifically, a higher
prevalence of a smoking history (P=0.014) and
diabetes mellitus (P=0.046) were observed in
the poor healing group. Additionally, osteoporo-
sis was more common in the poor healing group
compared to the healing group (P=0.003).
Comparison of fracture characteristics
No significant differences were found between
the healing and poor healing groups regarding
Risk factors and predictive model for non-healing
5769
Am J Transl Res 2025;17(7):5766-5778
Table 1.
Comparison of baseline data of patients
Data
Healing group (n=806)
Poor healing group (n=83)
t/x
2
P
Gender [n (%)]
0.088 0.767
Male
365 (45.29%)
39 (46.99%)
Female
441 (54.71%)
44 (53.01%)
Age (years)
68 ± 6
69 ± 6
1.028 0.304
Ethnicity (Han/Other) [n (%)]
742 (92.06%)
77 (92.77%)
0.053 0.819
BMI (kg/m
2
)
20.29 ± 6.43
19.61 ± 3.54
1.512 0.133
Smoking History [n (%)]
381 (47.27%)
51 (61.45%)
6.053 0.014
Diabetes Mellitus [n (%)]
383 (47.52%)
49 (59.04%)
3.996 0.046
Hypertension [n (%)]
445 (55.21%)
50 (60.24%)
0.772 0.380
Hyperlipidemia [n (%)]
438 (54.34%)
49 (59.04%)
0.669 0.413
Osteoporosis [n (%)]
329 (40.82%)
48 (57.83%)
8.917 0.003
Educational level [n (%)]
0.012 0.912
High school or below
539 (66.87%)
56 (67.47%)
Junior college or above
267 (33.13%)
27 (32.53%)
Monthly household income/person [n (%)]
0.033 0.855
<5000
448 (55.58%)
47 (56.63%)
≥5000
358 (44.42%)
36 (43.37%)
BMI: Body Mass Index.
Table 2.
Comparison of fracture characteristics of patients
Data
Healing group (n=806)
Poor healing group (n=83)
t/x
2
P
Fracture Type [n (%)]
0.303 0.582
Stable
414 (51.36%)
40 (48.19%)
Unstable
392 (48.64%)
43 (51.81%)
Garden Alignment Index [n (%)]
1.352 0.245
Ideal
423 (52.48%)
38 (45.78%)
Non-ideal
383 (47.52%)
45 (54.22%)
Posterior or Medial Wall Bone Defect [n (%)]
296 (36.72%)
44 (53.01%)
8.452 0.004
Cause of Fracture [n (%)]
1.175 0.556
Traffic Accident
262 (32.51%)
29 (34.94%))
Fall from Height
240 (29.78%)
20 (24.10%)
Fall
304 (37.72%)
34 (40.96%)
AO/OTA [n (%)]
0.382 0.536
A1.1-A2.1
418 (51.86%)
46 (55.42%)
A2.2-A3.3
388 (48.14%)
37 (44.58%)
ASA score [n (%)]
0.005 0.943
I/II
314 (38.96%)
32 (38.55%)
III/IV
492 (61.04%)
51 (61.45%)
Time to Weight Bearing (d)
5.182 0.023
≤15
409 (50.74%)
53 (63.86%)
>15
397 (49.26%)
30 (36.14%)
AO/OTA: Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association; ASA: American Society of Anesthesi-
ologists.
fracture type (P=0.582), Garden Alignment
Index (P=0.245), cause of fracture (P=0.556),
AO/OTA classification (P=0.536), or ASA score
(P=0.943) (
Table 2
). However, significant differ
-
Risk factors and predictive model for non-healing
5770
Am J Transl Res 2025;17(7):5766-5778
Table 3.
Comparison of blood test indicators [n (%)]
Index
Healing group (n=806)
Poor healing group (n=83)
t/x
2
P
Preoperative Hemoglobin (g/L)
0.051
0.822
<110
446 (55.33%)
47 (56.63%)
≥110
360 (44.67%
36 (43.37%)
Preoperative Albumin (g/L)
6.385
0.012
≤30
285 (35.36%)
41 (49.4%)
>30
521 (64.64%)
42 (50.6%)
Preoperative CRP (mg/L)
3.76 ± 1.51
4.23 ± 2.14
1.927
0.057
Preoperative IL-6 (pg/mL)
12.45 ± 3.52
13.32 ± 4.25
1.807
0.074
Preoperative Vitamin D Level (ng/mL)
23.21 ± 8.55
21.87 ± 7.32
1.378
0.168
Postoperative Hemoglobin (g/L)
3.524
0.060
<110
566 (70.22%)
50 (60.24%)
≥110
240 (29.78%)
33 (39.76%)
Postoperative Albumin (g/L)
6.149
0.013
≤30
278 (34.49%)
40 (48.19%)
>30
528 (65.51%)
43 (51.81%)
Postoperative CRP (mg/L)
2.73 ± 1.14
3.05 ± 1.53
1.856
0.067
Postoperative IL-6 (pg/mL)
10.55 ± 2.86
11.31 ± 3.91
1.718
0.089
Postoperative Vitamin D Level (ng/mL)
22.15 ± 8.23
20.76 ± 7.18
1.479
0.140
CRP: C-reactive Protein; IL-6: Interleukin-6.
ences were noted for posterior or medial wall
bone defects and time to weight bearing. A
higher proportion of patients in the poor heal-
ing group had posterior or medial wall bone
defects compared to the healing group (P=
0.004). Additionally, the poor healing group
showed a significantly greater proportion of
patients who began weight bearing within 15
days post-surgery (P=0.023).
Comparison of blood test indicators
The poor healing group exhibited a higher per
-
centage of patients with preoperative albumin
levels ≤30 g/L (P=0.012, χ
2
=6.385) and post-
operative albumin levels ≤30 g/L (P=0.013,
χ
2
=6.149) compared to the healing group
(
Table 3
). No significant differences were found
in preoperative hemoglobin levels (P=0.822),
postoperative hemoglobin levels (P=0.060),
preoperative CRP (P=0.057), preoperative IL-6
(P=0.074), preoperative Vitamin D levels (P=
0.168), postoperative CRP (P=0.067), postop-
erative IL-6 (P=0.089), or postoperative Vitamin
D levels (P=0.140) between the two groups.
Comparison of surgical-related factors
The healing group had a higher percentage of
patients treated with proximal femoral nail anti
-
rotation (PFNA) compared to the poor healing
group, while the poor healing group had a high-
er proportion of patients treated with DHS
(P=0.012) (
Table 4
). No significant differences
were observed between the groups in terms of
time from fracture to surgery (P=0.398), surgi-
cal time (P=0.132), or intraoperative blood loss
(P=0.389).
Comparison of preoperative psychological and
cognitive tests
The preoperative psychological and cognitive
evaluations revealed some trends approaching
statistical significance between the healing
and poor healing groups (
Table 5
). Specifically,
Stroop Test results showed a trend toward sig-
nificance, with the poor healing group scor-
ing slightly higher than the healing group
(t=1.961, P=0.053). No significant differences
were found for other measures: PSQ scores,
WCST results, and Alternative Use Task per-
formance showed no significant differences
between the two groups.
Correlation analysis
The correlation analysis of various indicators
identified several significant factors for non
-
union after internal fixation in elderly patients

Risk factors and predictive model for non-healing
5771
Am J Transl Res 2025;17(7):5766-5778
Table 4.
Analysis of surgical related factors
Factor
Healing group (n=806)
Poor healing group (n=83)
t/x
2
P
Time from Fracture to Surgery (d)
2.30 ± 0.55
2.34 ± 0.42
0.849
0.398
Internal fixation method
6.317
0.012
PFNA
456 (56.58%)
35 (42.17%)
DHS
350 (43.42%)
48 (57.83%)
Surgical Time (h)
49.89 ± 5.60
50.65 ± 4.18
1.517
0.132
Intraoperative Blood Loss (ml)
125.61 ± 23.18
128.46 ± 29.07
0.866
0.389
PFNA: Proximal femoral nail antirotation; DHS: Dynamic hip screw.
Table 5.
Comparison of preoperative psychological and cognitive evaluation of patients
Test
Healing group (n=806)
Poor healing group (n=83)
t
P
PSQ Score
13.08 ± 3.15
13.65 ± 3.24
1.570
0.117
Stroop Test Result
49.52 ± 6.31
51.17 ± 7.42
1.961
0.053
WCST results
22.13 ± 2.55
21.54 ± 3.14
1.661
0.100
Alternative Use Task Performance
78.32 ± 10.32
76.45 ± 11.24
1.558
0.120
PSQI Score
6.83 ± 2.21
7.27 ± 2.44
1.687
0.092
PSQ: Parent Symptom Questionnaire; WCST: Wisconsin Card Sorting Test; PSQI: Pittsburgh Sleep Quality Index.
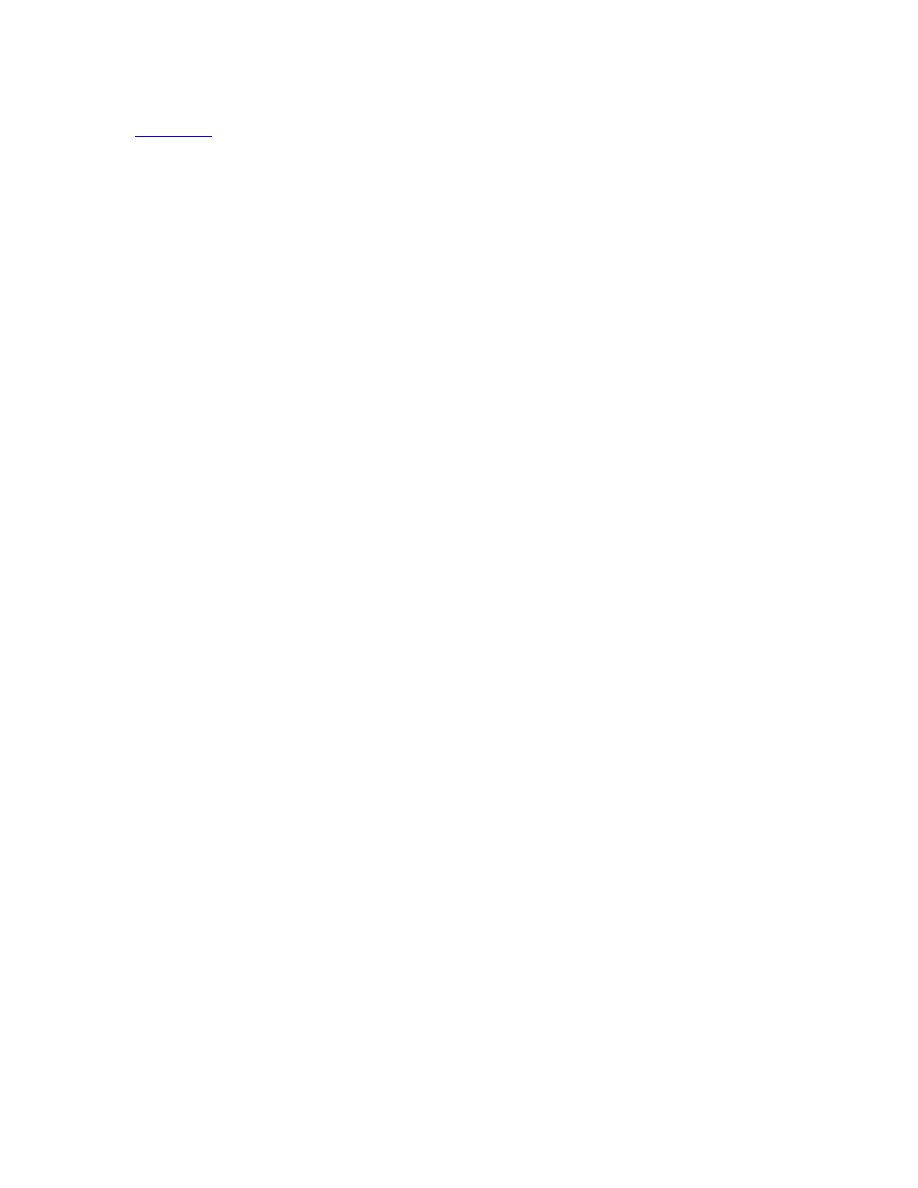
Figure 1.
Correlation analysis of various indicators with nonunion after internal fixation in elderly patients with inter
-
trochanteric femoral fractures. PFNA: Proximal femoral nail antirotation; DHS: Dynamic hip screw.
with intertrochanteric femoral fracture (
Figure
1
). Smoking history (rho=0.083, P=0.014) and
diabetes mellitus (rho=0.067, P=0.046) were
positively correlated with nonunion. Osteopo-
Risk factors and predictive model for non-healing
5772
Am J Transl Res 2025;17(7):5766-5778
Table 6.
Univariate logistic regression analysis of risk factors
Coefficient
Std Error
Wald
P
OR
CI Lower CI Upper
Smoking History
0.575
0.236
2.435
0.015
1.778
1.125
2.849
Diabetes Mellitus
0.465
0.234
1.986
0.047
1.592
1.010
2.536
Osteoporosis
0.687
0.234
2.943
0.003
1.988
1.262
3.162
Posterior or Medial Wall Bone Defect
0.665
0.232
2.868
0.004
1.944
1.235
3.071
Preoperative Albumin (g/L) (≤30/>30)
0.539
0.239
2.256
0.024
1.715
1.081
2.768
Postoperative Albumin (g/L) (≤30/>30)
0.579
0.232
2.501
0.012
1.785
1.132
2.813
Time to Weight Bearing (d) (≤15/>15)
0.569
0.232
2.455
0.014
1.767
1.119
2.785
Internal fixation method
-0.580
0.233
2.487
0.013
0.560
0.352
0.882
Table 7.
Multivariate logistic regression analysis of risk factors
Coefficient
Std Error Wald
P
OR
OR CI Lower OR CI Upper
Smoking History
0.559
0.244
2.292 0.022 1.750
1.084
2.823
Diabetes Mellitus
0.432
0.243
1.779 0.075 1.541
0.957
2.480
Osteoporosis
0.720
0.241
2.992 0.003 2.055
1.282
3.294
Posterior or Medial Wall Bone Defect
0.675
0.239
2.818 0.005 1.964
1.228
3.140
Preoperative Albumin (g/L) (≤30/>30)
0.418
0.248
1.690 0.091 1.520
0.935
2.469
Postoperative Albumin (g/L) (≤30/>30)
0.515
0.240
2.150 0.032 1.674
1.047
2.678
Time to Weight Bearing (d) (≤15/>15)
0.568
0.241
2.361 0.018 1.765
1.101
2.829
Internal fixation method
-0.664
0.242 -2.748 0.006 0.515
0.321
0.827
rosis (rho=0.100, P=0.003) and posterior or
medial wall bone defects (rho=0.098, P=0.004)
also demonstrated positive correlations with
nonunion. Nutritional status, indicated by albu-
min levels, showed that low preoperative (≤30
g/L) and postoperative albumin levels were cor-
related with nonunion (rho=0.076, P=0.023;
rho=0.085, P=0.011, respectively). Additionally,
early weight bearing (≤15 days) correlated po-
sitively with nonunion (rho=0.083, P=0.013).
Conversely, the choice of internal fixation meth
-
od showed a negative correlation with non-
union (rho=-0.084, P=0.012). These results
highlight several clinical and surgical factors
significantly associated with nonunion risk in
the studied population.
Univariate logistic regression analysis
The univariate logistic regression analysis iden-
tified several significant risk factors for non-
healing in elderly patients with intertrochanter-
ic fractures following internal fixation surgery
(
Table 6
). Smoking history was associated with
an increased odds of non-healing, with an odds
ratio (OR) of 1.778 (P=0.015). Similarly, diabe-
tes mellitus was significantly associated with
non-healing, with an OR of 1.592 (P=0.047).
Osteoporosis was a strong predictor, with an
OR of 1.988 (P=0.003). The presence of poste-
rior or medial wall bone defects significantly
increased the risk of non-healing, with an OR of
1.944 (P=0.004). Patients with preoperative
albumin levels ≤30 g/L had higher odds of non-
healing (P=0.024), as did those with postopera-
tive albumin levels ≤30 g/L (P=0.012). Early
weight-bearing (≤15 days) was also associated
with increased odds of non-healing (P=0.014).
In contrast, the use of PFNA was associated
with reduced odds of non-healing (P=0.013),
suggesting it has a protective role against
nonunion.
Multivariate logistic regression analysis
The multivariate logistic regression analysis
identified several independent risk factors sig
-
nificantly associated with non-healing in elder-
ly patients with intertrochanteric fracture post-
internal fixation surgery (
Table 7
). Smoking his-
tory remained a significant risk factor, with an
OR of 1.750 (P=0.022). Osteoporosis emerg-
ed as a strong predictor, with an OR of 2.055
(P=0.003). The presence of posterior or medial
wall bone defects was also significantly associ
-
ated with non-healing risk, with an OR of 1.964
Risk factors and predictive model for non-healing
5773
Am J Transl Res 2025;17(7):5766-5778
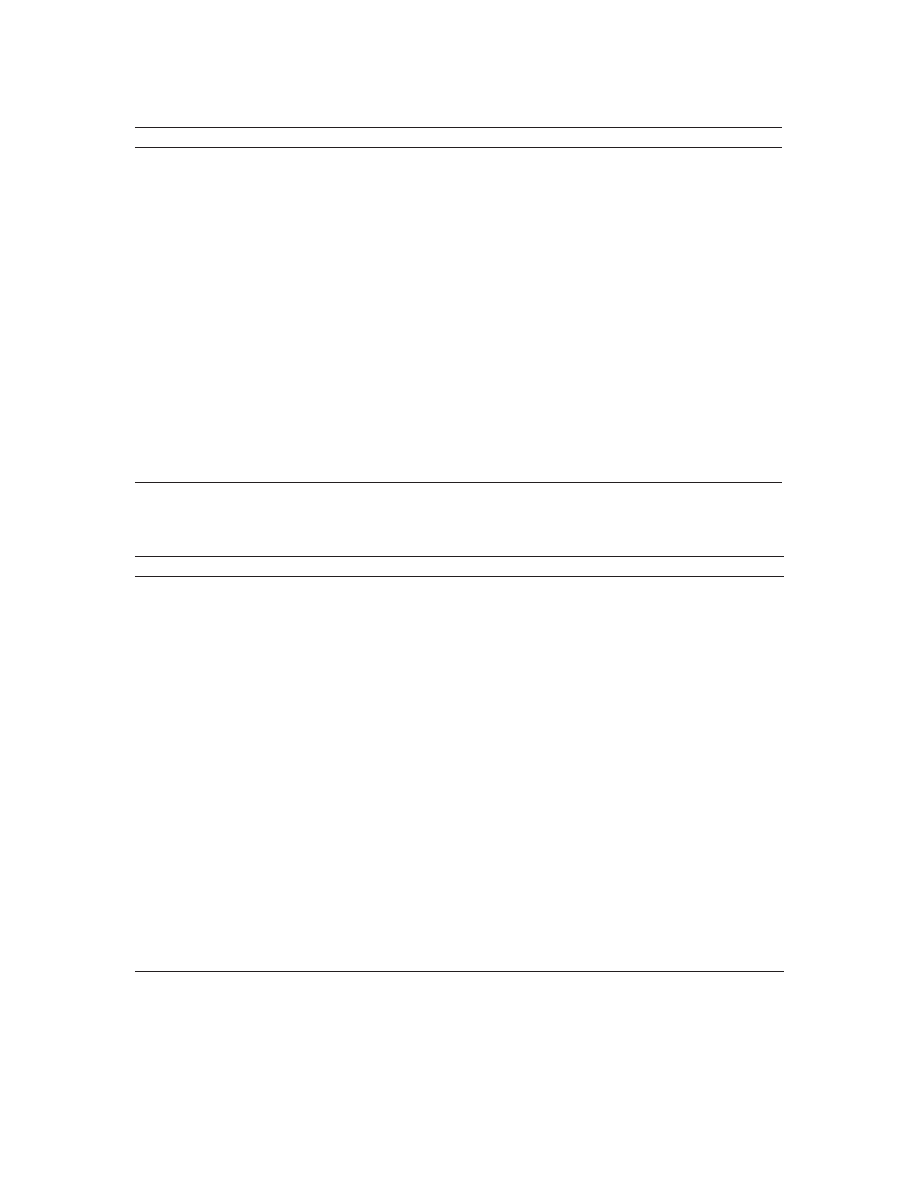
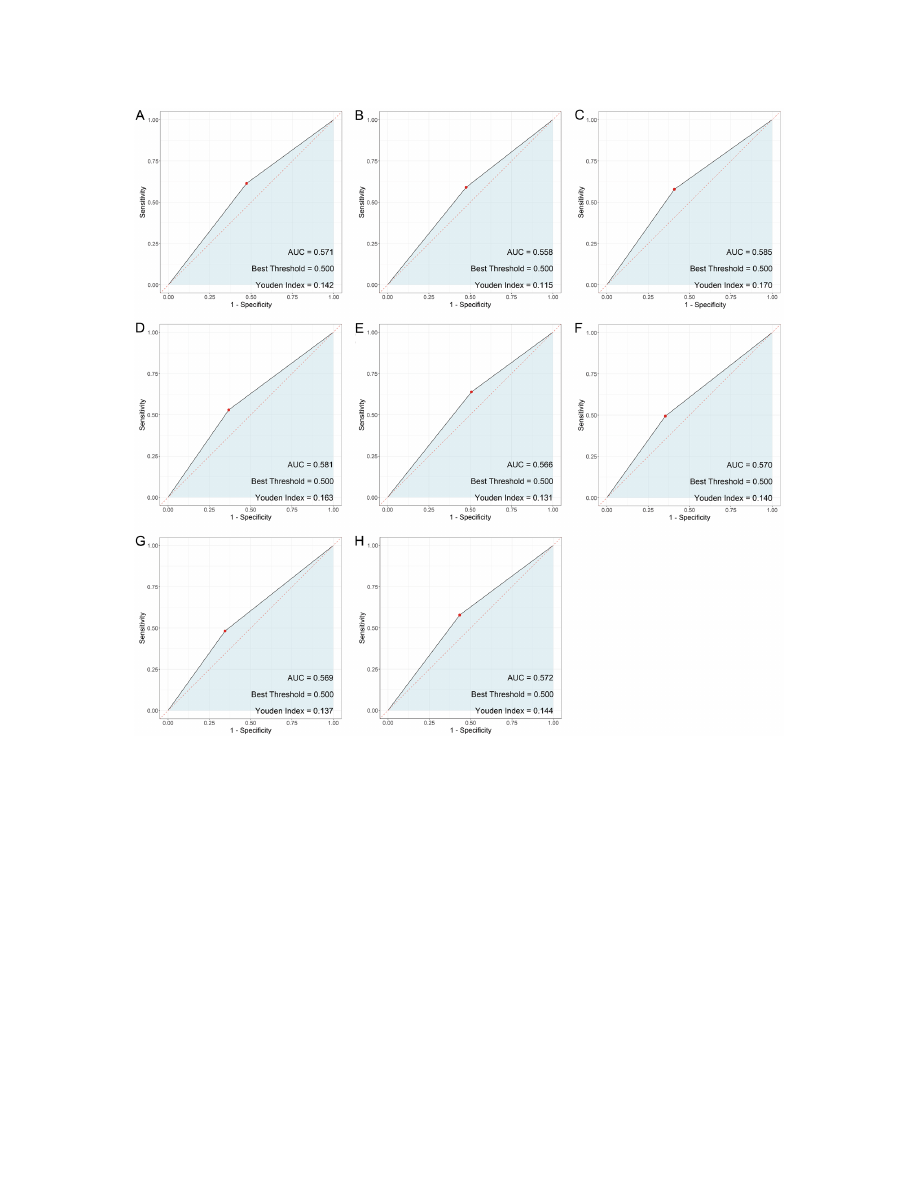
Figure 2.
Predictive value of each in-
dex for non-union in elderly patients
with intertrochanteric fracture after
internal fixation. A. Smoking History;
B. Diabetes Mellitus; C. Osteoporo-
sis; D. Posterior or Medial Wall Bone
Defect; E. Time to Weight Bearing
(≤15 d/>15 d); F. Postoperative Al
-
bumin (≤30 g/L/>30 g/L); G. Post
-
operative Hemoglobin (≤30 g/L/>30
g/L); H. Internal fixation method.
(P=0.005). While preoperative albumin levels
showed a trend towards significance, postop
-
erative albumin levels ≤30 g/L were significant
-
ly associated with non-healing (P=0.032). Early
weight bearing (≤15 days) was associated with
an increased risk of non-healing (P=0.018).
Conversely, the use of a PFNA significantly
reduced the likelihood of non-healing, with an
OR of 0.515 (P=0.006). Diabetes mellitus
(P=0.075) and preoperative albumin levels
(P=0.091) did not reach statistical significan-
ce in this multivariate analysis, indicating that
their effects may be confounded by other vari-
ables in the model. These findings emphasize
the importance of managing targeted risk fac-
tors to optimize patient outcome.
ROC analysis
The analysis of predictive values for non-union
in elderly patients with intertrochanteric frac-
tures following internal fixation surgery high
-
lights variable predictive capabilities among
different factors (
Figure 2
). Osteoporosis dem-
onstrated the highest sensitivity (0.578) and a
specificity of 0.592, with an AUC of 0.585, indi
-
cating moderate discrimination between heal-
ing outcomes. Posterior or medial wall bone
defects exhibited a specificity of 0.633 and
sensitivity of 0.530, with an AUC of 0.581.
Smoking history, diabetes mellitus, and preop-
erative albumin levels displayed similar predic-
tive performance, with AUCs of 0.571, 0.558,
Risk factors and predictive model for non-healing
5774
Am J Transl Res 2025;17(7):5766-5778
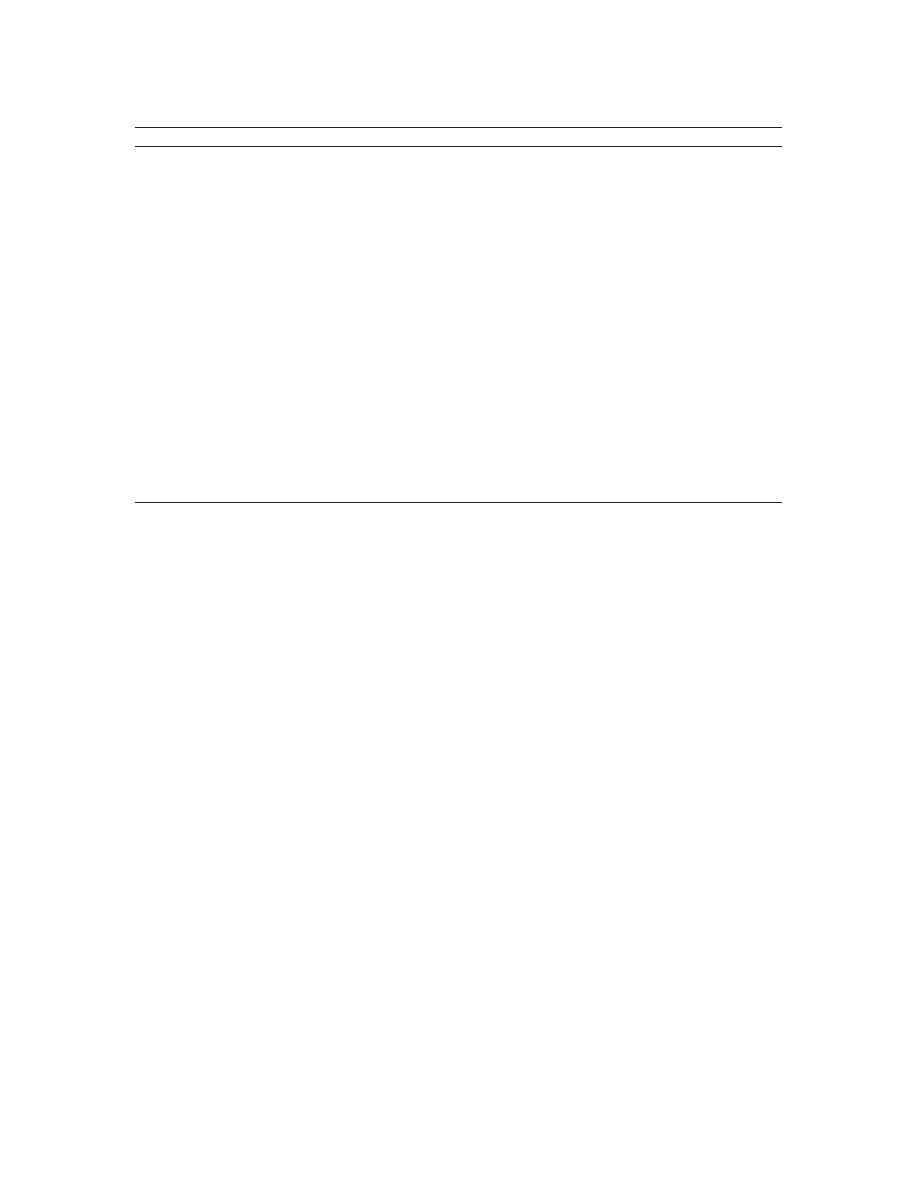
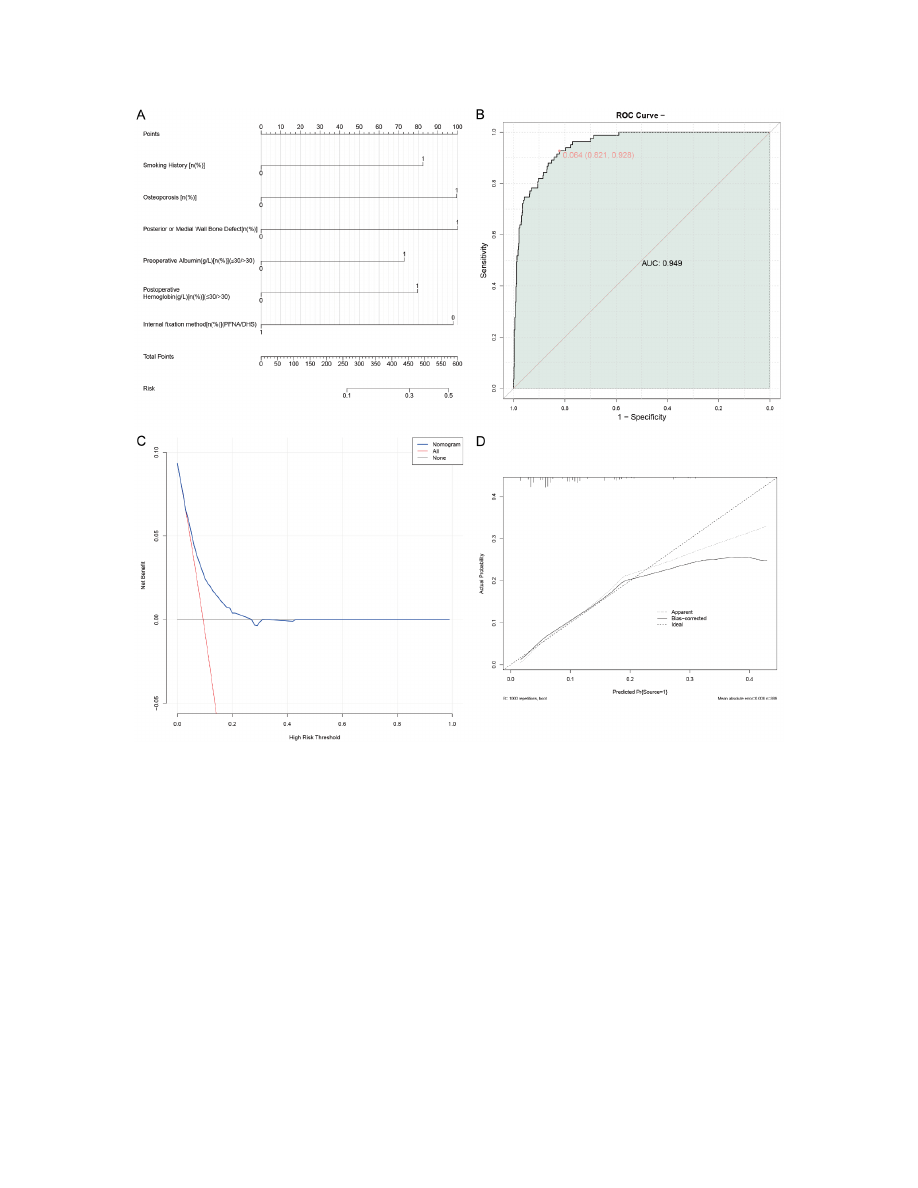
Figure 3.
The joint prediction model for non-union in elderly patients following internal fixation for intertrochanteric
femoral fractures. A. Nomogram; B. Joint ROC Curve; C. DCA; D. Calibration Curves. ROC: receiver operator charac-
teristic; AUC: area under the curve; DCA: Decision Curve Analysis.
and 0.566, respectively, and Youden indices
indicating limited predictive separation. Post-
operative albumin levels and time to weight-
bearing also had moderate specificities (0.646
and 0.655, respectively), but lower sensitivi-
ties, yielding AUCs of 0.570 and 0.569. The
internal fixation method revealed balanced
sensitivity and specificity, with values of 0.578
and 0.566, respectively, and an AUC of 0.572.
Overall, these indicators provide moderate pre-
dictive information, suggesting that a multifac-
torial approach is necessary for accurately pre-
dicting non-union risk. The F1 scores, par-
ticularly for osteoporosis (0.209) and bone
defects (0.208), suggest a need for further
refinement in predictive modeling to enhance
clinical utility.
Joint prediction model
This study combined various risk factors af-
fecting non-healing in elderly patients with
intertrochanteric femoral fracture after internal
fixation to construct a comprehensive predic
-
tive model for post-surgical non-union (
Figure
3
). The nomogram, based on multivariate re-
gression analysis, accurately predicted individ-
ualized risk scores, with strong performance

Risk factors and predictive model for non-healing
5775
Am J Transl Res 2025;17(7):5766-5778
confirmed through internal validation. The
model achieved an AUC of 0.949, indicating
exceptional predictive value. The Decision
Curve Analysis (DCA) demonstrated that our
model provided a higher net benefit across a
wide range of clinically relevant probability
thresholds, suggesting that it can effectively
identify high-risk patients. This allows clinicians
to make informed decisions about targeted pre-
ventive intervention. Calibration curves showed
excellent agreement between predicted proba
-
bilities and observed outcomes, confirming the
model’s reliability. Overall, these results affirm
the robustness and clinical utility of our predic-
tive model for post-surgical non-union.
Discussion
This study investigated risk factors for non-
healing in elderly patients with intertrochanter-
ic femoral fractures treated with internal fixa
-
tion and developed a predictive model to
identify patients at increased risk. Our results
indicate that a history of smoking, osteoporo-
sis, and posterior or medial wall bone defects
are significantly associated with poor healing
after surgery. These findings enhance our un-
derstanding of the factors that may compro-
mise healing and underscore the importance
of comprehensive management strategies for
these patients.
The significant association between smoking
and non-healing aligns with existing literature,
which shows that smoking impairs bone heal-
ing [21, 22]. Cigarette toxinsincluding nicotine,
disrupt osteoblast activity and reduce blood
flow to the fracture site, hindering bone repair
[22]. Smoking also impedes angiogenesis and
reduces oxygen levels at the healing site, both
of which are crucial for successful fracture
repair [23]. Chronic smoking weakens the im-
mune response, potentially delaying the early
inflammatory phase that is essential for in-
itiating healing [24]. Collectively, these effects
emphasize the importance of smoking cessa-
tion as part of orthopedic care for improving
healing outcomes.
Osteoporosis emerged as another significant
predictor in our analysis. Characterized by
reduced bone density and weakened bone
structure, osteoporosis is a known contributor
to fracture non-union [25]. The pathophysiology
of osteoporosis involves an imbalance in bone
remodeling, with increased osteoclast activity
and decreased osteoblast function [26]. This
imbalance leads to porous bone architecture
and diminished mechanical stability, both of
which are essential for successful fracture
healing [27]. Additionally, the reduced osteo
-
genic potential in osteoporotic bone can result
in delayed callus formation and inferior callus
quality, further complicating the healing pro-
cess [28]. Pharmacologic management of os-
teoporosis, such as bisphosphonates to inhibit
osteoclast-mediated bone resorption or newer
anabolic treatments, may be beneficial in pro
-
moting fracture healing.
Our analysis also identified posterior or medial
wall bone defects as significant factors contrib
-
uting to poor healing outcome. The integrity of
these bone walls is crucial for maintaining the
stability and alignment of fracture fragments
during the healing process [29]. Defects in
these areas can compromise mechanical sup-
port and lead to increased micromovement at
the fracture site, which impedes bone regener-
ation [30]. Biomechanically, stability during the
initial inflammatory stage of bone healing is
critical, as it sets the stage for subsequent
repair and remodeling [31]. Addressing these
defects surgically, using techniques such as
bone grafting or reinforced fixation methods,
may improve outcome by providing enhanced
mechanical stability.
Moreover, our findings indicate that both preop
-
erative and postoperative serum albumin le-
vels are important indicators of nutritional sta-
tus and correlate with healing outcome. Hy-
poalbuminemia, a marker of poor nutritional
status, is critical for collagen synthesis, wound
healing, and overall tissue regeneration [32].
Adequate nutrition supports cellular processes
essential for healing, including osteogenic cell
proliferation and effective immune function
[33]. Therefore, optimizing nutrition through
dietary interventions or supplementation, sh-
ould be emphasized preoperatively and main-
tained throughout recovery to facilitate optimal
healing.
Interestingly, early postoperative weight-bear-
ing was identified as a risk factor for non-union.
While early mobilization can reduce complica-
tions such as deep vein thrombosis and en-
hance physical conditioning, excessive loading
on an unstable fracture can hinder bone heal-

Risk factors and predictive model for non-healing
5776
Am J Transl Res 2025;17(7):5766-5778
ing [34]. This highlights the need for a balanced
approach to postoperative management, where
a tailored, patient-specific weight-bearing pro
-
tocol is essential to ensure that movement
does not compromise the integrity of the heal-
ing bone [35].
The type of internal fixation used during sur-
gery also significantly affected healing. Our
data showed that PFNA reduced the risk of
non-union compared to DHS. The PFNA design
provides better stability by controlling rotation
and distributing force more effectively along
the bone [36]. This enhanced stability likely
explains the lower non-union rates observed
with PFNA, suggesting that surgeons should
carefully consider the fixation method and its
ability to maintain bone stability when planning
an operation.
Our predictive model, with a high AUC of 0.949,
demonstrates that these risk factors collective-
ly offer robust predictive value. The model’s
high predictive accuracy reinforces the con-
cept that fracture healing is multifactorial, with
clinical, biochemical, and surgical factors all
contributing to the risk of non-union. Imple-
menting this model in clinical practice may help
identify high-risk patients earlier, allowing for
timely interventions based on each patient’s
specific risks and potentially improving out-
come.
While this study provides valuable insights, its
limitations must be acknowledged. The retro-
spective nature of the analysis may have over-
looked factors not captured in the data. Fu-
ture research should involve larger, prospective
studies tracking patients over time to validate
these findings. Such studies could also investi
-
gate additional factors, such as genetic mark-
ers or specific surgical techniques, to further
refine the model.
In conclusion, our research illustrated that sev-
eral modifiable and non-modifiable risk factors
significantly influence healing outcomes in
elderly patients undergoing internal fixation for
intertrochanteric femoral fracture. Key strate-
gies to reduce the risk of non-healing include
smoking cessation, osteoporosis management,
optimal surgical technique selection, and en-
suring adequate nutrition. These interventions
are crucial for improving both functional out-
comes and quality of life in these vulnerable
patients. Further advancements in predictive
models will enable more personalized care, ulti-
mately enhancing surgical success.
Acknowledgements
This study was supported by the Wuxi Municipal
Health Commission (No. M202246).
Disclosure of conflict of interest
None.
Address correspondence to:
Jijun Zhao, Depart-
ment of Orthopedics, Wuxi People’s Hospital, No.
299 Qingyang Road, Wuxi 214023, Jiangsu, China.
E-mail: zhaojijun2024@126.com
References
[1]
Zhang J, Fan X, Zheng Y, Wu J and Yuan X. Intra-
venous application of tranexamic acid in intra
-
medullary nailing for the treatment of geriatric
intertrochanteric fractures: a systematic re-
view and meta-analysis. BMC Musculoskelet
Disord 2023; 24: 614.
[2]
Yang F, Li X, Zhao L and Yang Q. Dual-screw
versus single-screw cephalomedullary nails for
intertrochanteric femoral fractures: a system-
atic review and meta-analysis. J Orthop Surg
Res 2023; 18: 607.
[3] Yalın M, Golgelioglu F and Key S. Intertrochan
-
teric femoral fractures: a comparison of clini-
cal and radiographic results with the proximal
femoral intramedullary nail (PROFIN), the anti-
rotation proximal femoral nail (A-PFN), and the
InterTAN Nail. Medicina (Kaunas) 2023; 59:
559.
[4]
Xie W, Shi L, Zhang C, Cui X, Chen X, Xie T,
Zhang S, Chen H and Rui Y. Anteromedial corti
-
cal support reduction of intertrochanteric frac-
tures-a review. Injury 2024; 55: 111926.
[5] Wang H, Chen M, Wu Y and Ge J. 3D printing in
intertrochanteric fractures of the femur. Mi-
nerva Pediatr (Torino) 2023; 75: 627-629.
[6]
Tang Y, Wang D, Wang L, Xiong W, Fang Q, Lin
W and Wang G. The PFNA in treatment of inter-
trochanteric fractures with or without lateral
wall fracture in elderly patients: a retrospective
cohort study. Eur J Med Res 2023; 28: 380.
[7]
T J and Kwek EBK. Are intertrochanteric frac-
tures evolving? Trends in the elderly popula-
tion over a 10-year period. Clin Orthop Surg
2022; 14: 13-20.
[8] Sniderman J, Vivekanantha P, Shah A, Safir O,
Wolfstadt J and Kuzyk P. Hemiarthroplasty for
unstable intertrochanteric hip fractures: a
matched cohort study. J Arthroplasty 2023;
38: 1522-1527.

Risk factors and predictive model for non-healing
5777
Am J Transl Res 2025;17(7):5766-5778
[9]
Sivakumar A, Rickman M and Thewlis D. Gait
biomechanics after proximal femoral nailing of
intertrochanteric fractures. J Orthop Res 2023;
41: 862-874.
[10]
Sekimura T, Son SJ and Lee C. Reverse obliq-
uity intertrochanteric femur fractures: techni-
cal tips to avoid failure. J Orthop Trauma 2023;
37: S19-S25.
[11] Schroeder JD, Turner SP and Buck E. Hip frac
-
tures: diagnosis and management. Am Fam
Physician 2022; 106: 675-683.
[12] Rincón-Hoyos JA, Gómez-Ramírez JF, Cuesta-
Montoya JS, Lara-Garavito AM, Muñoz-Medina
SE and Castro-Dangond AJ. Treatment of inter-
trochanteric fractures using cephalomedullary
nail: one or two cephalic screws? Injury 2023;
54 Suppl 6: 110625.
[13]
Ricci WM. Stability of intertrochanteric femur
fractures. J Orthop Trauma 2023; 37: S1-S4.
[14]
Parikh K, Kandemir U and Agarwal A. Intertro-
chanteric hip fractures: pearls and pitfalls in
managing difficult fractures. Instr Course Lect
2023; 72: 375-387.
[15] Nherera L, Trueman P, Horner A, Watson T and
Johnstone AJ. In reply to the letter to the editor
regarding “Comparison of a twin interlocking
derotation and compression screw cephalom-
edullary nail (InterTAN) with a single screw
derotation cephalomedullary nail (proximal
femoral nail antirotation): a systematic review
and meta-analysis for intertrochanteric frac-
tures”. J Orthop Surg Res 2022; 17: 354.
[16]
Morrison J and Morrison M. Management of
hip fractures. Crit Care Nurs Clin North Am
2024; 36: 575-584.
[17]
Mayor J, Birgel V, Clausen JD, Aktas G, Sehm-
isch S, Einfeldt AK, Giannoudis V, Abdelaal
AHK and Liodakis E. Lessons learned from bio
-
mechanical studies on cephalomedullary nails
for the management of intertrochanteric frac-
tures. A scoping review. Injury 2024; 55:
111180.
[18]
Garden RS. Stability and union in subcapital
fractures of the femur. J Bone Joint Surg Br
1964; 46: 630-647.
[19] Gu J, He S and Wang L. Analysis of one-year
postoperative mortality and risk factors of el-
derly patients with intertrochanteric fractures
after PFNA. Niger J Clin Pract 2022; 25: 1557-
1562.
[20]
Fjeld A, Fülling T, Bula P and Bonnaire F. Func-
tional outcomes and perceived quality of life
following fixation of femoral neck fractures in
adults from 18 to 69 years using dynamic hip
screw (DHS) and an additional anti-rotation
screw- a retrospective analysis of 53 patients
after a mean follow-up time of 4 years. Eur J
Trauma Emerg Surg 2022; 48: 1893-1903.
[21] Matsubara T, Soma K, Yamada I, Fujita H, Yo
-
shitani J, Oka H, Okada H and Tanaka S. Offset
nail fixation for intertrochanteric fractures im
-
proves reduction and lag screw position. PLoS
One 2022; 17: e0276903.
[22] Maffulli N and Aicale R. Proximal femoral frac
-
tures in the elderly: a few things to know, and
some to forget. Medicina (Kaunas) 2022; 58:
1314.
[23] Lu Y, Huang Q, Xu Y, Ren C, Sun L, Dong W, Li
M, Xue H, Li Z, Zhang K, Ma T and Wang Q.
Predictors of long-term mortality after intertro-
chanteric fractures surgery: a 3-year retrospec-
tive study. BMC Musculoskelet Disord 2022;
23: 472.
[24]
Liu D, Yu X, Chen L and Wang Z. Ipsilateral
femoral neck, intertrochanteric and acetabular
fractures with posterior dislocation of the hip:
a case report and literature review. Medicine
(Baltimore) 2023; 102: e36275.
[25] Liao CS, He FZ, Li XY and Han PF. Proximal
femoral nail antirotation versus InterTan nail
for the treatment of intertrochanteric frac-
tures: a systematic review and meta-analysis.
PLoS One 2024; 19: e0304654.
[26] Li H, Wang D, Zhang W, Xu G, Xu C, Zhang H,
Zhang L, Li J and Tang P. Does computer-assist-
ed orthopaedics system (ADAPT system) im-
prove outcomes of intertrochanteric hip frac-
tures? Injury 2023; 54: 1047-1054.
[27]
Lähdesmäki M, Ylitalo AA, Karjalainen L, Uim-
onen M, Mattila VM and Repo JP. Intramedul-
lary nailing of intertrochanteric femoral frac-
tures in a level i trauma center in finland: what
complications can be expected? Clin Orthop
Relat Res 2024; 482: 278-288.
[28] Katsuyama Y, Okuda Y, Kanamura H, Sasaki K,
Saito T and Nakamura S. Surgical versus con-
servative treatment of greater trochanteric
fractures with occult intertrochanteric frac-
tures: retrospective cohort study. Injury 2023;
54: 111055.
[29] Izawa Y, Futamura K, Murakami H, Shirakawa
T, Nishida M, Baba T and Tsuchida Y. Risk fac-
tors for over-telescoping in reverse oblique in-
tertrochanteric fractures. Eur J Orthop Surg
Traumatol 2023; 33: 1101-1107.
[30] Huff S, Henningsen J, Schneider A, Hijji F,
Froehle A and Krishnamurthy A. Differences
between intertrochanteric and femoral neck
fractures in resuscitative status and mortality
rates. Orthop Traumatol Surg Res 2022; 108:
103231.
[31] Huang J and Wei Q. Comparison of helical
blade versus lag screw in intertrochanteric
fractures of the elderly treated with proximal
femoral nail: a meta-analysis of randomized-
controlled trials. Jt Dis Relat Surg 2022; 33:
695-704.

Risk factors and predictive model for non-healing
5778
Am J Transl Res 2025;17(7):5766-5778
[32] Hongku N, Woratanarat P, Nitiwarangkul L,
Rattanasiri S and Thakkinstian A. Fracture fixa
-
tion versus hemiarthroplasty for unstable in-
tertrochanteric fractures in elderly patients: a
systematic review and network meta-analysis
of randomized controlled trials. Orthop Trau-
matol Surg Res 2022; 108: 102838.
[33] Hantouly AT, Salameh M, Toubasi AA, Salman
LA, Alzobi O, Ahmed AF and Ahmed G. The role
of cerclage wiring in the management of sub-
trochanteric and reverse oblique intertrochan-
teric fractures: a meta-analysis of comparative
studies. Eur J Orthop Surg Traumatol 2023;
33: 739-749.
[34]
Green J, Watson JT, Shaheen P and Kuldjanov
D. Geriatric intertrochanteric fractures: what is
the optimal follow-up period? J Orthop Trauma
2023; 37: 557-561.
[35] Goodnough LH, Wadhwa H, Tigchelaar SS, De
-
Baun MR, Chen MJ, Graves ML and Gardner
MJ. Indications for cement augmentation in
fixation of geriatric intertrochanteric femur
fractures: a systematic review of evidence.
Arch Orthop Trauma Surg 2022; 142: 2533-
2544.
[36] Duan W, Liang H, Fan X, Zhou D, Wang Y and
Zhang H. Research progress on the treatment
of geriatric intertrochanteric femur fractures
with proximal femur bionic nails (PFBNs). Or
-
thop Surg 2024; 16: 2303-2310.